In this article:
This article is part 2 of a series about specificity testing. Be sure to read part 1, an introduction to the series.
Summary
Even though monoclonal antibodies are prized for their specificity, 1 in 3 lead candidates exhibit off-target binding. Because off-target interactions are so common and their safety consequences so large, we need accurate methods for identifying them. Specificity testing during preclinical development typically involves one or both of two technologies: tissue cross-reactivity (TCR) studies, which have been in use since the 1980s, and cell-based protein arrays, which have emerged in the last decade or so. Other methods, including tissue microarrays and spotted protein microarrays, have limitations that make them inappropriate for preclinical safety testing. While early FDA guidance focused on TCR, recent documents have named protein arrays as an appropriate alternative.
Why is specificity testing important?
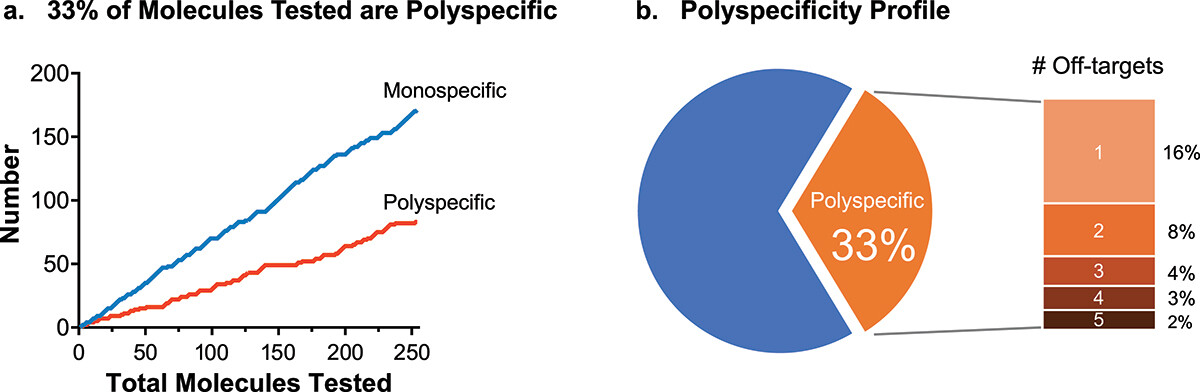
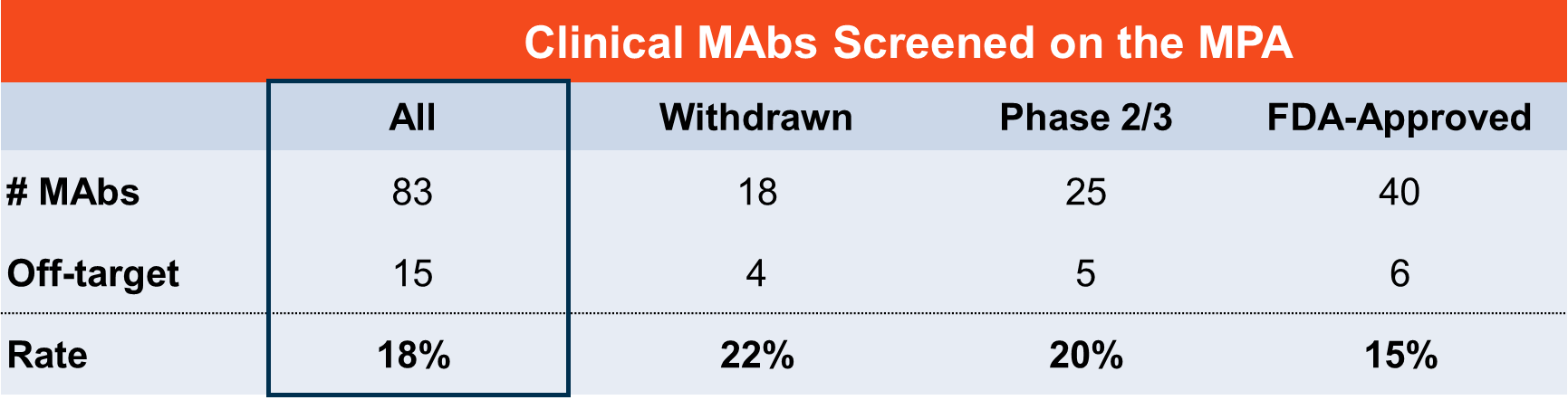
Monoclonal antibodies (Mabs) are prized for their exquisite specificity—especially compared to their small-molecule counterparts. Yet a study of therapeutic MAbs in development and on the market showed that 1 in 3 lead candidates exhibited off-target binding (Norden et al., 2024).
Given the potential consequences of off-target interactions—on patient safety, drug efficacy, pharmacokinetics—it’s essential to have accurate methods for identifying them during preclinical development. That way, we can advance only the safest, most-selective drugs to the clinic.
In this article, we’ll break down the methods that are currently available for preclinical specificity testing and describe how FDA guidance in this realm has changed over time.
What is off-target binding?
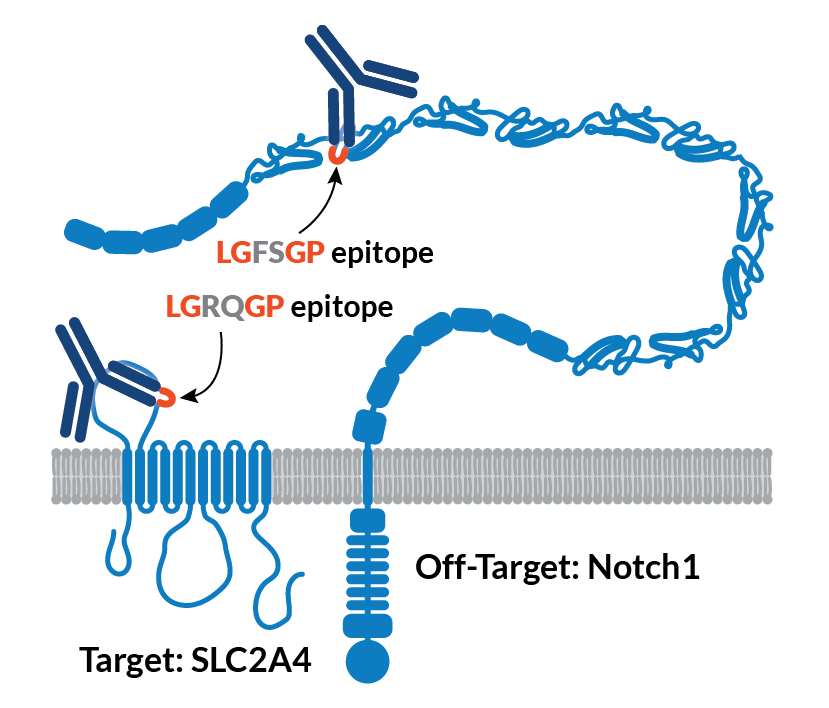
Off-target binding, also known as cross-reactivity or polyspecificity, is CDR-mediated binding to one or more proteins other than the intended target. Sometimes the off-target is a member of the same protein family, but most often it’s a completely unrelated protein and thus extremely difficult to predict.
That’s in contrast to polyreactivity, which refers to a more general type of antibody stickiness—an antibody developability challenge in its own right. There are well-known methods for detecting polyreactivity, though we won’t discuss them here.
For a deeper discussion of polyreactivity and polyspecificity, see Cunningham et al., 2021.
What off-target specificity testing methods are currently available?
While the FDA has yet to qualify any tools for evaluating biotherapeutic specificity, several technologies exist for this purpose. Specificity testing during preclinical development typically involves tissue cross-reactivity studies, cell-based protein arrays, or both. Other methods, including tissue microarrays and spotted protein microarrays, have limitations that make them inappropriate for regulatory submissions.
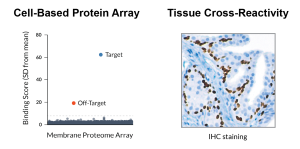
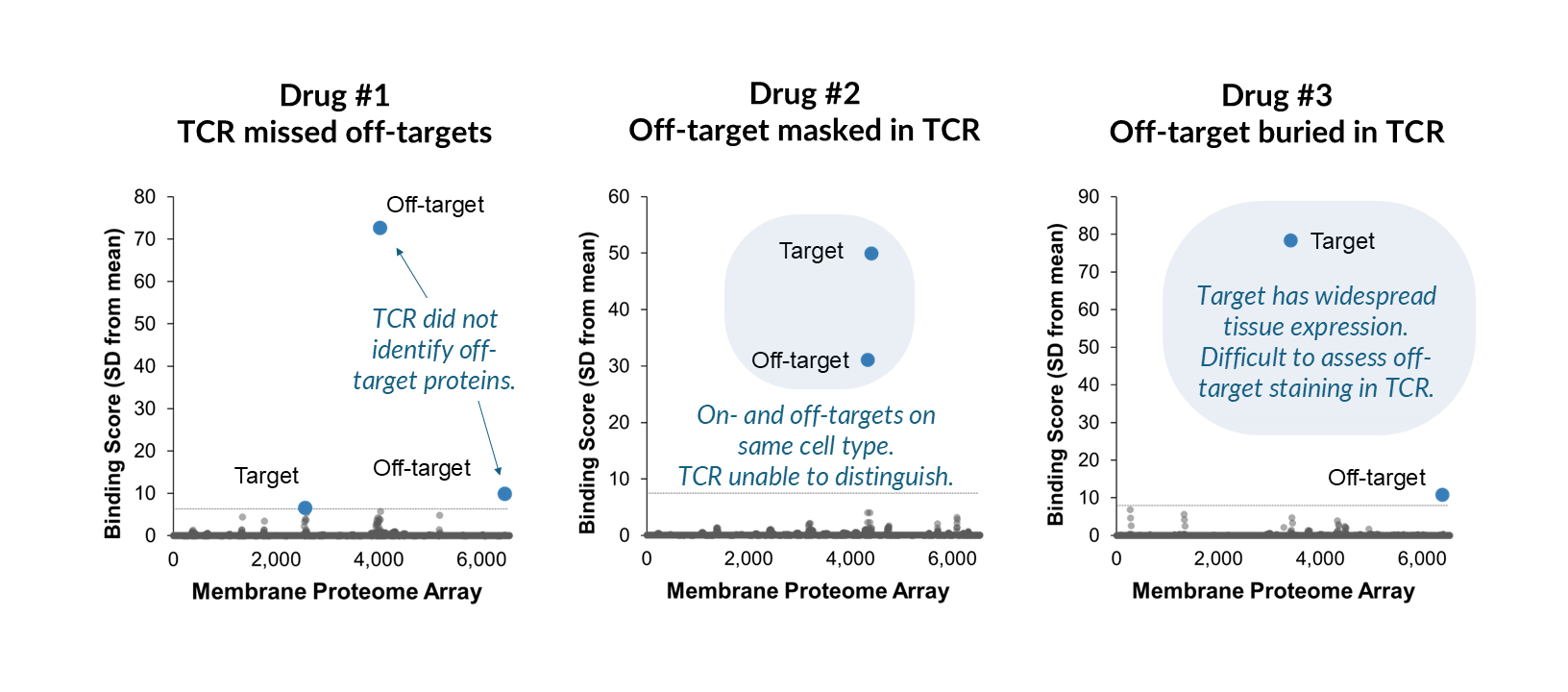
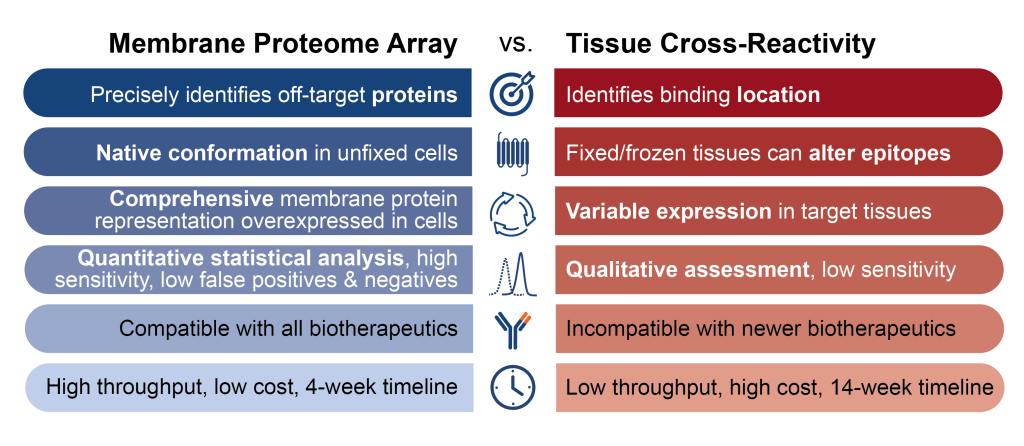
Tissue cross-reactivity (TCR) studies were developed in the early 1980s to meet the need for specificity testing for biologics. This in vitro assay uses immunohistochemistry (IHC) to reveal antibody binding across a panel of human tissue samples from three individual donors. Results are interpreted by a pathologist, who looks for unexpected off-target binding and previously unknown sites of on-target binding. While TCR data is still widely used in regulatory submissions, no validation studies have been published to quantify its sensitivity, false-negative or false-positive rate, or outcome-based results.
Tissue microarrays (TMAs) consist of up to 1,000 small tissue samples attached to a slide. As with TCR, IHC reveals binding locations within tissues. TMAs are available for purchase, making testing easier, faster, and less costly than TCR studies. However, because the small samples do not faithfully represent all elements of the original tissue, and because TMAs typically are not interpreted by a pathologist, they are less rigorous than TCR. TMAs are best suited as a research tool for investigating target expression profiles and screening for specificity earlier in development.
Spotted protein arrays consist of recombinant proteins from bacteria, yeast, or eukaryotic cell lysates spotted onto a solid surface. While these tools typically represent a high percentage of human proteins and come at an affordable price point, they sacrifice protein integrity. Limitations include a lack of post-translational modifications due to non-mammalian cell production, altered protein conformations, protein denaturation, and unnatural surface interactions. Most importantly, spotted protein arrays do not accurately represent multi-pass membrane proteins (the targets of most biotherapeutics), which typically require a lipid bilayer to maintain their native structure.
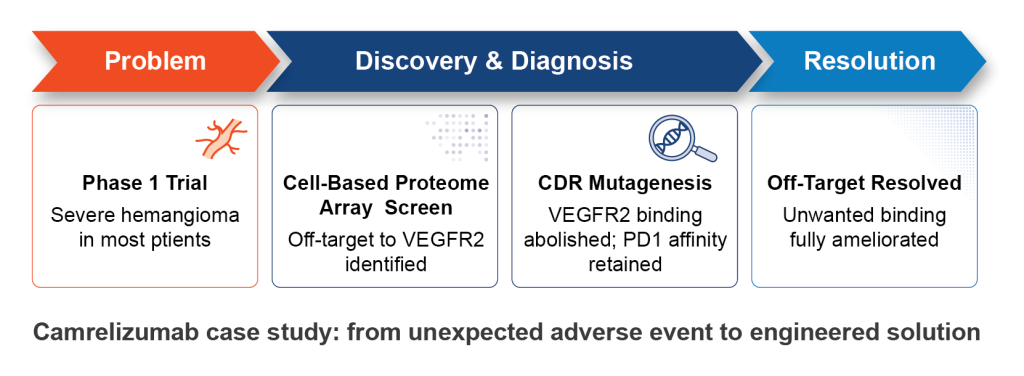
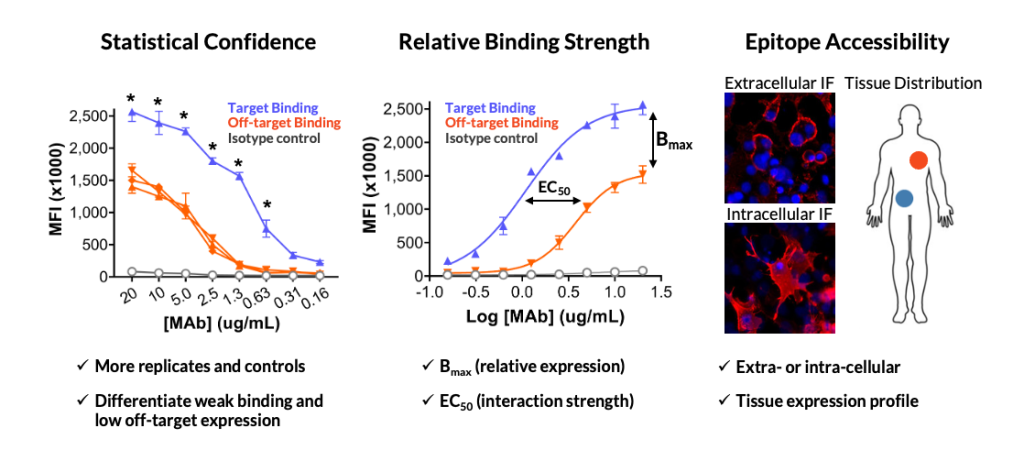
Cell-based protein arrays (CBPAs) have emerged in the last decade or so as a faster, less costly, and more precise alternative to TCR studies. CBPAs, such as the Membrane Proteome Array, are a higher-throughput in vitro technology using vertebrate (usually human) cells that overexpress thousands of individual proteins in their natural conformation with post-translational modifications. Binding is evaluated by either IHC or flow cytometry. While TCR reveals only the locations of off-target binding, CBPAs identify the off-target proteins across the human membrane proteome, enabling detailed follow-up study. CBPAs are commonly used early in drug development for lead selection and later for regulatory submissions.
How has FDA guidance for specificity testing changed over time?
When it comes to selecting specificity testing tools for preclinical safety studies, drug developers generally follow guidance for regulatory submission provided by the FDA and similar agencies around the globe.
Regulatory documents first described TCR in 1983. In the mid-1990s, regulatory agencies, including the EMA and FDA, began formally recognizing the need to assess specificity testing. The FDA formally recommended TCR in 1997 as the best available tool at the time.
Regulatory agencies have long anticipated that new specificity testing technologies would emerge, potentially enhancing or even replacing TCR data. In its 1997 guidance the FDA stated, “appropriate newer technologies should be employed as they become available and validated.” Similarly, in 2011, ICH biotherapeutic guidance stated, “other technologies can be employed in place of IHC techniques to demonstrate target/binding site distribution.”
In January 2024, the FDA for the first time delineated specific alternative methods to TCR studies. In their new guidance document for CAR-T therapeutic development, they named “protein arrays” as an appropriate specificity testing method. This brief mention formalized a shift that had already begun. Because TCR lacks the sensitivity required for CAR-T testing, drug developers had already been using cell-based protein arrays for this purpose, and the FDA had already accepted this data in dozens of IND submissions.
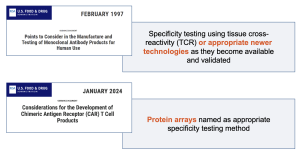
1FDA, 1997. Points to Consider in the Manufacture and Testing of Monoclonal Antibody Products for Human Use
2FDA, 2024. Considerations for the Development of Chimeric Antigen Receptor (CAR) T Cell Products
Most recently, the FDA signaled an even greater shift toward advancing human-relevant new-approach methodologies (NAMs). In April of 2025, the FDA released a “Roadmap to reduced animal testing in preclinical safety studies,” outlining its plan to leverage NAMs to replace, reduce, and refining animal testing. Essential to this vision, the FDA has plans to advance human-relevant methods like organoid systems, computational modeling, and advanced in vitro assays.
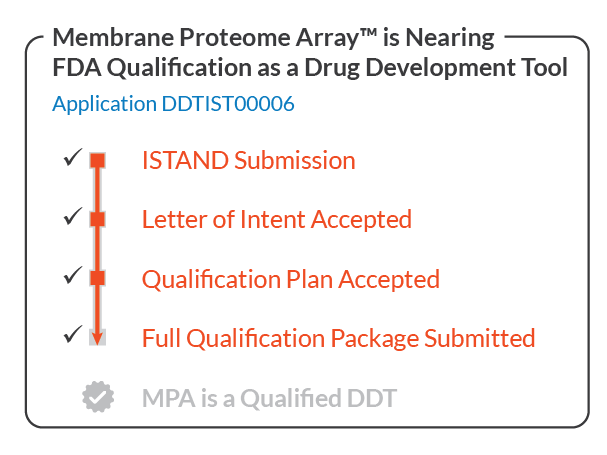
The Membrane Proteome Array is a high-throughput in vitro cell-based screening assay that embodies the FDA’s vision. It screens the full human membrane proteome with objective, quantitative results rather than the subjective tissue analysis methods that have defined the field for 40 years. In the coming articles, we’ll explore what that means in practice.
Looking ahead
For the next article in this series, we’ll dig deeper into TCR studies, their limitations, and how much they influence drug development decisions (spoiler: not much).